

MASLD and FIB-4 in Primary Care: The Patients Not to Miss
- 5 days ago
- 3 min read
Why This Matters
Metabolic dysfunction-associated steatotic liver disease (MASLD) is now one of the most common liver conditions encountered in primary care.
As rates of obesity and type 2 diabetes continue to rise, incidental fatty liver on ultrasound has become an everyday finding. The challenge is no longer identifying patients with steatosis — it is identifying the minority at risk of advanced fibrosis and liver-related complications.
Fortunately, most patients with MASLD will never develop cirrhosis.
The key question is:
Who has fibrosis?
Five Things I Want You To Remember
Fat on ultrasound does not predict prognosis.
Fibrosis predicts outcomes.
Most patients with MASLD can be managed in primary care.
FIB-4 is the recommended first-line fibrosis assessment tool.
Cardiovascular disease remains the leading cause of death in most patients with MASLD.
What Has Changed?
Then
Fatty liver was often regarded as a benign incidental finding.
Referral decisions were largely based on liver enzyme abnormalities.
Many patients were referred directly for specialist review.
Now
Fibrosis is recognised as the major determinant of liver-related outcomes.
FIB-4 is recommended as the first-line risk stratification tool.
Most patients can remain under primary care.
Referral is increasingly focused on identifying advanced fibrosis rather than steatosis.
The Most Important Concept
Fibrosis Predicts Outcomes, Not Steatosis
When reviewing an ultrasound report, it is tempting to focus on:
Mild steatosis
Moderate steatosis
Severe steatosis
However, the amount of fat in the liver does not reliably predict future liver-related outcomes.
Patients with severe steatosis may never develop advanced liver disease.
Conversely, patients with relatively modest steatosis may progress to significant fibrosis.
Specialist Insight
The question is not:
"How much fat is present?"
The question is:
"Is fibrosis developing?"
Who Should Be Assessed?
Consider fibrosis assessment in patients with:
Type 2 diabetes
Obesity
Metabolic syndrome
Persistently abnormal liver function tests
Steatosis identified on imaging
Clinical Pearl
More than two-thirds of patients with type 2 diabetes have underlying fatty liver disease.
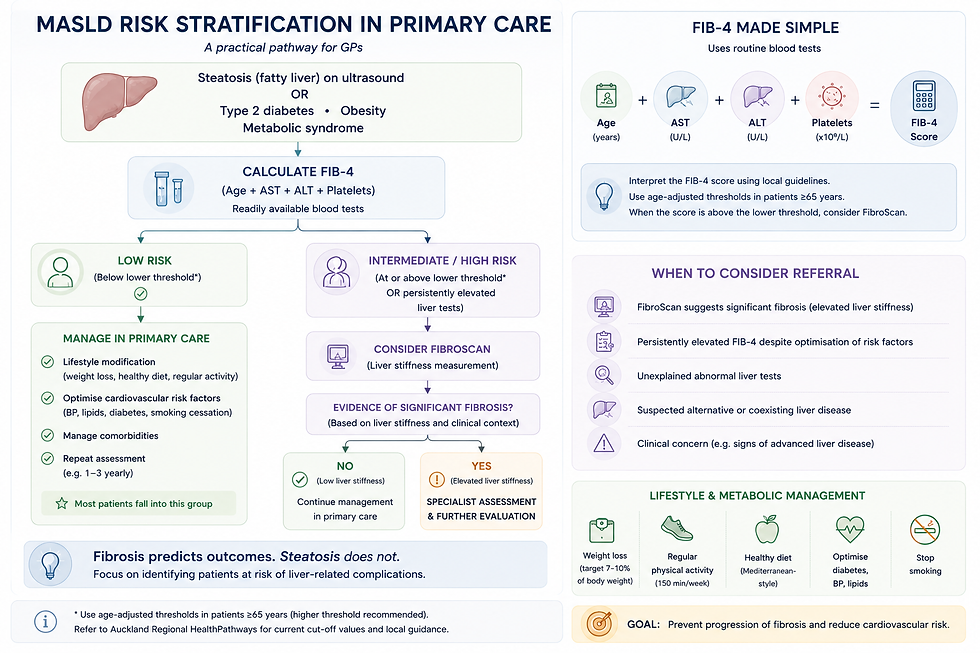
A Practical Approach to FIB-4
FIB-4 uses:
Age
AST
ALT
Platelet count
These are investigations already available in most primary care settings.
Low Risk
FIB-4 below the lower threshold
Management:
Lifestyle intervention
Weight loss
Cardiovascular risk reduction
Repeat assessment periodically
Most patients can remain under primary care.
Intermediate or High Risk
Elevated FIB-4
Management:
Consider FibroScan
Assess for alternative liver disease
Consider specialist referral
Age Matters
One important update is that FIB-4 becomes less specific with increasing age.
For patients aged 60 years and older:
A higher threshold of approximately 2.0 is recommended before triggering further investigation.
This reduces unnecessary referrals and FibroScans in older adults.
The Role of FibroScan
FibroScan provides non-invasive assessment of liver stiffness.
Liver Stiffness <8 kPa
Low likelihood of advanced fibrosis.
Most patients can remain under primary care.
Liver Stiffness ≥8 kPa
Consider specialist assessment and further evaluation.
Remember
FibroScan is a risk stratification tool.
It does not replace clinical judgement.
Before You Label Someone With MASLD
Perform a basic liver screen at least once.
Consider:
Hepatitis B
Hepatitis C
Haemochromatosis
Autoimmune liver disease
These conditions can coexist with fatty liver and may alter management significantly.
Common Pitfall
Do not assume every abnormal liver test in an overweight patient is due to MASLD.
What Is My Patient Most Likely To Die From?
This often surprises patients.
For most individuals with early-stage MASLD:
The greatest long-term health risk is cardiovascular disease.
Not cirrhosis.
Not liver cancer.
Management should therefore focus on:
Weight loss
Diabetes optimisation
Blood pressure control
Lipid management
Smoking cessation
Physical activity
Specialist Insight
Many MASLD consultations are really cardiovascular prevention consultations in disguise.
GLP-1 Therapies and MASLD
GLP-1 receptor agonists and dual incretin therapies are increasingly relevant in MASLD management.
Benefits include:
Weight loss
Improved glycaemic control
Reduced liver fat
Cardiovascular risk reduction
Current evidence suggests that weight loss remains the major driver of liver benefit.
Clinical Pearl
A sustained weight loss of approximately 7–10% of total body weight can improve steatohepatitis and may improve fibrosis.
When Should I Refer?
Consider specialist assessment if:
FibroScan ≥8 kPa
FIB-4 remains elevated
Unexplained abnormal liver tests
Concern regarding alternative liver disease
Evidence of advanced fibrosis or cirrhosis
Referral should be directed by fibrosis risk rather than the degree of steatosis reported on ultrasound.
Five Things I Want You To Remember
Fibrosis predicts outcomes, not steatosis.
Calculate FIB-4 before referring most patients.
Most patients with MASLD can remain under primary care.
Always exclude alternative liver disease at least once.
Cardiovascular disease remains the major long-term risk.
Useful Resources
For Clinicians
GastroConsult Elevated Ferritin Resource
GastroConsult Abnormal Liver Function Tests Resource
Disclaimer
This resource is intended for healthcare professionals and reflects available evidence at the time of publication. Clinical decisions should be individualised according to patient circumstances, local referral pathways, and specialist advice where appropriate.


Comments